MIT engineers just cracked a 30-year-old problem, they kept the transplanted insulin-producing cells alive inside the body without suppressing the immune system.
This problem has haunted medicine for decades. To understand that, let’s first consider a situation, you wake up, grab your insulin pen, and inject yourself before breakfast. You’ll do this again at lunch, followed by dinner, again before bed. For millions of people living with type 1 diabetes, this four-times-daily ritual is just the price of staying alive.
But what if the “four-times-daily ritual” is not required? That’s the question biomedical researchers were trying to solve for years. And this week, scientists at MIT published findings that suggest they’ve finally found a path forward, one involving a tiny, wireless implant about the size of a postage stamp that could handle insulin production automatically, right inside your body.
So why hasn’t this “simple transplant fix” worked?
Logically, transplanting pancreatic islet cells, the insulin-producing powerhouses of our pancreas, can work and doctors have tried this approach, however, the problem is immune rejection.
Our body treats transplanted cells like invaders, so patients who receive islet transplants have traditionally had to take immunosuppressive drugs, these powerful medications can dampen their immune system’s ability to attack the foreign cells. But that’s not the end of it, these drugs come with nasty side effects like:
- increased infection risk
- kidney damage
- for some patients, the burden becomes worse than managing diabetes itself
Researchers like Daniel Anderson at MIT have been hunting for a solution that could keep transplanted cells alive without destroying the immune system in the process.
A Protective Bubble With an Oxygen Factory
Anderson’s team started thinking something different, they didn’t invent a new type of cell, they invented a container smart enough to protect them.
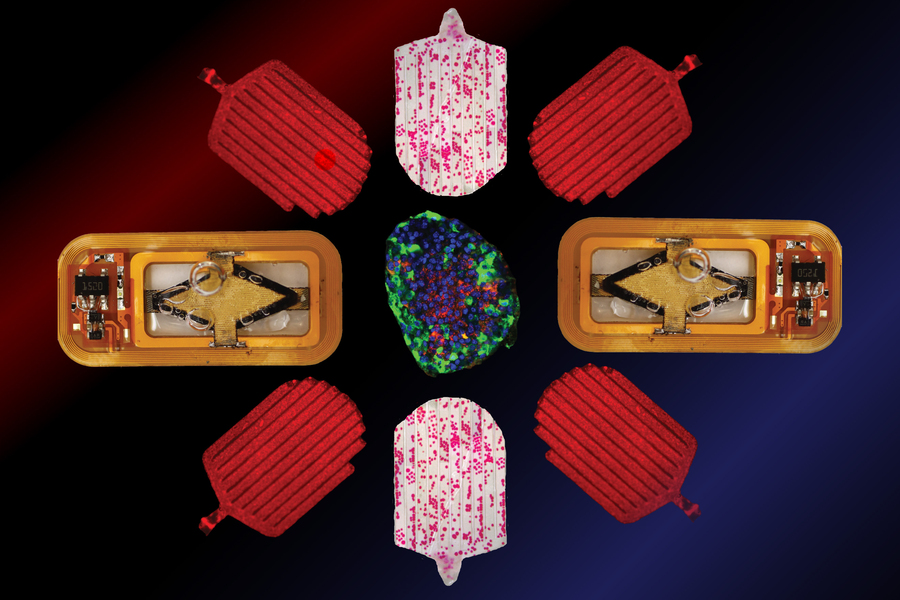
So, the idea is, a thin, flexible device, about the size of a postage stamp, filled with a soft gel. Inside that gel, thousands of insulin-producing islet cells are cozy and protected. They are sealed off from the immune system’s attack but still connected to the body’s needs.
So obviously, the real innovation behind the tech is, the device doesn’t just sit there passively, it actively keeps the cells alive.
We know that cells are metabolically greedy, they need oxygen. When you seal them away inside a protective device, that oxygen can be hard to get to them. Previous attempts at cell encapsulation ran into this problem. The protective barrier that kept the immune system out also kept oxygen from getting in.
So this time the MIT team built an oxygen generator inside the device itself.
They used a proton-exchange membrane, the device taps into water vapor that’s naturally abundant in your body. It then splits that vapor into hydrogen and oxygen. The hydrogen harmlessly diffuses away while the oxygen gets stored in a small chamber connected to the islet cells through a thin, oxygen-permeable membrane.
It’s like planting a tiny oxygen factory right next to the cells that need it.
How the Device Runs Without Wires or Batteries
Now the device needs electricity to run that oxygen generator. But you can’t have wires sticking out of your body, that’s an infection risk and a quality-of-life problem.
So the team made it wireless.
They made an external antenna to be placed on the skin for transmitting energy to the implant, which powers the oxygen-generating system, which means, no batteries, no wires, no daily maintenance. The user would wear a small patch-like antenna, and the implant does its job silently in the background.
In their latest study, the researchers optimized this wireless power transfer. By improving the device’s electronics, they managed to send more power to the oxygen generator, which meant it could produce more oxygen, which meant the cells could survive longer and produce more insulin.
The Results: From 30 Days to 90 Days
In experiments with mice and rats, cells remained alive and functional for at least 90 days after implantation. During that time, they produced enough insulin to keep the animals’ blood sugar levels in a healthy range.
That might sound like a modest timeframe, but it’s huge in translational medicine. If something only works for about a month, it just shows that the idea might be possible. But if it keeps working for three months, that’s much more important. It means the main problem has likely been solved, and the cells aren’t just barely surviving, they’re actually doing well in that environment.
And they’re not done yet. The team is now working toward keeping the implants functional for two years or longer. Anderson says,
“Long-term survival of the islets is an important goal. The cells, if they’re in the right environment, seem to be able to survive for a long time”.
The Takeaway
The majority of the people suffering from Type 1 diabetes spend decades injecting insulin, pricking their fingers to monitor blood sugar, and living with the constant background anxiety of a disease that never stops.
Current islet cell transplants work, but they’re reserved for the most severely affected patients, those who can’t manage their blood sugar safely even with aggressive insulin therapy and they require lifelong immune suppression.
This implant could change that math. If a device can protect cells from immune rejection without immune suppression, it becomes accessible to far more patients. A three-month device wouldn’t solve it alone, but a one-year or two-year device would be transformative. That’s the difference between a burdensome medical procedure and a practical life-changing treatment.
In their paper, the team mentions exploring whether this same approach could deliver cells that produce other useful proteins such as, antibodies, enzymes, and clotting factors. I mean just think about it, implants manufacturing on demand medication, rather than requiring patients to receive infusions in a hospital every few weeks.
“We think that these technologies could provide a long-term way to treat human disease by making drugs in the body instead of outside of the body”, Anderson said.
For patients with hemophilia who need clotting factors, or those with rare enzyme deficiencies, or anyone requiring expensive, frequent biologic treatments, this could be revolutionary.
Of course, the current research is working on mice and rats and translating from rodent models to human patients is always a jump, bodies are more complex, immune systems are more nuanced, and scale matters.
But for the millions of people who spend their lives managing blood sugar, the possibility of a device that handles it for them, without daily injections or immune-suppressing medications, is worth waiting for.
MIT’s implant is one example but I’m sure we’ll see similar innovations in cancer treatment (devices that release drugs locally), heart disease (implants that monitor and adjust pacing), and neurological disorders (brain implants that read and interpret neural signals).
This isn’t science fiction. It’s happening now, incrementally, in labs and operating rooms around the world.
Source: MIT News
Frequently Asked Questions
What is MIT’s new insulin implant and how does it work?
MIT engineers developed a wireless implant about the size of a postage stamp containing thousands of insulin-producing islet cells protected by a soft gel. The device encapsulates cells in a thin, flexible container sealed from the immune system. Inside, a proton-exchange membrane converts naturally abundant water vapor in the body into oxygen and hydrogen, with the oxygen delivered to cells through a permeable membrane. An external skin patch antenna wirelessly powers the oxygen-generating system, eliminating the need for batteries, wires, or daily maintenance.
Why have insulin cell transplants failed for 30 years?
Transplanted pancreatic islet cells trigger immune rejection because the body treats them as foreign invaders. Previous solutions required lifelong immunosuppressive drugs that cause severe side effects including increased infection risk, kidney damage, and conditions worse than diabetes itself. The fundamental barrier was that protective encapsulation blocked oxygen from reaching cells, causing them to die. MIT solved both the immune rejection and oxygen delivery problems simultaneously.
How long do the implanted cells survive and produce insulin?
In mouse and rat experiments, implanted cells remained alive and functional for at least 90 days, producing sufficient insulin to maintain healthy blood sugar levels throughout that period. The MIT team is currently working to extend implant longevity to two years or longer. Researchers note that 90-day survival represents a major milestone—it demonstrates the core problem is solved and cells are thriving, not merely surviving short-term.
What are the advantages compared to current type 1 diabetes treatment?
Current treatment requires four daily insulin injections, frequent blood sugar monitoring, and constant anxiety about glucose management. Existing islet cell transplants work but require lifelong immune-suppressing medications with serious side effects and are only available to severely affected patients. This wireless implant would eliminate daily injections, prevent immune system suppression, require no wires or batteries, and be compatible with normal daily activities while the device operates silently in the background.
When will this technology be available to patients?
The technology is currently in the animal testing phase (mice and rats). Translating to human patients typically requires 5-10 years for clinical trials and regulatory approval. MIT researchers are focused on extending implant functionality from 90 days toward 1-2 year longevity before human trials begin. A one-year device would be immediately practical; a two-year device would be transformative for diabetes management.
Could this implant technology treat diseases other than diabetes?
Yes. MIT is exploring the same encapsulation and wireless power approach to deliver therapeutic proteins including antibodies, enzymes, and clotting factors. Potential applications include hemophilia (clotting factor deficiencies), rare genetic enzyme deficiencies, and chronic conditions requiring expensive hospital infusions. This approach could enable the body to manufacture needed medications on-demand instead of requiring frequent hospital-based biologic treatments.
What is the oxygen-generating mechanism and why is it critical?
The device contains a proton-exchange membrane that harvests water vapor naturally present in the body. It electrochemically splits water vapor (H₂O) into hydrogen and oxygen molecules. Hydrogen harmlessly diffuses away while oxygen is stored in a chamber connected to encapsulated islet cells through an oxygen-permeable membrane. This “oxygen factory” solves the critical problem that plagued previous cell encapsulation attempts: protective barriers that blocked immune rejection also blocked oxygen diffusion, causing cell death. MIT’s integrated oxygen generation enables long-term cell survival within the sealed protective environment.